Anatomy and ideal proportion :
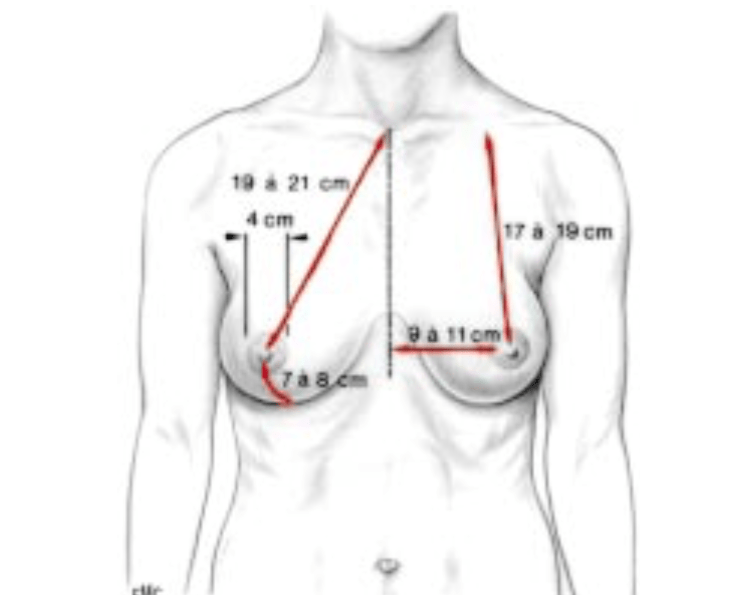
The ideal breast is 10-12 cm wide and the 2 nipples, centered in the middle of the breast, are about 20 cm apart (variable according to thorax width and morphology of the patient). The areola, with an ideal diameter of 38-45 mm, should be located 20 cm from the top of the sternum or halfway between the shoulder (acromion) and the elbow (epicondyle) and the distance between the nipple and the submammary fold should be about 7 cm.
Breast augmentation can be performed by fat transfer (lipofilling) or by silicone implant.
The lipofilling technique is reserved for patients who have sufficient fat reserves in the thighs, hips, abdomen and inner knees. The patient must be a non-smoker: in normal circumstances, 30% of the volume of the fat injected will be resorbed and for smokers, the loss often represents 50-80%. Patients who have an empty breast in the neckline or a ptosis (drooping) of the breast are bad candidates for lipofilling.
On the other hand, fat transfer can be used in combination with breast prostheses (hydride breast augmentation) to mask the rim of the prosthesis or to fill in the cleavage for patients with a large inter-mammary gap.
Breast implants :
Round or anatomical?
Breast implants can be round or anatomical, i.e. pear-shaped. Anatomical implants are of interest to patients who already have a round cleavage and who want a very natural result of the shape of the breast, but a natural result can also be obtained with a round implant. The natural effect depends on the shape, the location of the pocket that will be created for the implant and the extent of the insertion of the pectoral muscle on the sternum.
Low, moderate, high profile?
The profile is the distance between the base (flat part) and the top of the prosthesis: there are low, moderate and high profiles. The higher the profile, the greater the forward projection. The high profile prostheses are the most suitable for patients who wish to have a round cleavage. Dr. Lucas will choose the appropriate profile with you according to the shape and volume desired, but also according to the measurements of the width of your thorax.
Saline or silicone?
The prosthesis can be filled with saline water (saline) or silicone called cohesive (if the prosthesis is ruptured, the silicone does not leak but remains inside the prosthesis). Each has its advantages and disadvantages, but silicone has the advantage of being more natural to the touch. Dr. Lucas uses the latest generation of silicone prostheses (Sebbin ® or Mentor ®).
Smooth or textured surface?
Macrotextured prostheses (Biocell Allergan®), never used by Dr. Lucas, were recently withdrawn from the market because they are a risk factor in the development of large cell anaplastic lymphoma. Polyurethane-coated implants are not recommended.
Size
Dr. Lucas will guide you in choosing the size of the prosthesis, depending on the shape and size desired. On average, it takes 120-150 ml (or cc) to gain one cup size.
Retro-glandular or retro-muscular?
The prosthesis can be placed in front of (retroglandular) or behind the muscle (retro-muscular). Prostheses can be placed in front of the muscle for patients with good “coverage”, i.e., sufficient tissue thickness, whereas in thin patients it is preferable to place the prosthesis under the muscle, otherwise the edges of the prosthesis may be too pronounced and this could be unsightly. It is technically more difficult surgically to place prostheses behind the muscle, but in the long term the retro-muscular prostheses age better aesthetically, especially after breastfeeding which empties the mammary gland that covered the prosthesis.
Incision
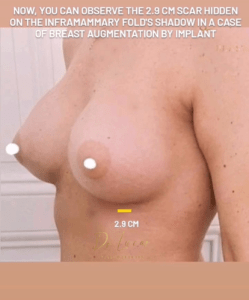
There are 3 main approaches for inserting a breast prosthesis: axillary (armpit), peri-areolar (semi-circular in the colored part of the nipple) or submammary. The axillary route is attractive because no scar is visible on the breast but requiring an endoscope and the use of Kellerfunnel to insert a silicone prosthesis, the cost increases significantly. The peri-areolar approach is feasible, if the diameter of the areola is more than 35 mm. Dr. Lucas most often uses the submammary route (in the fold under the breast) using a minimally invasive technique: 2.5-3.5 cm scar, hidden in the natural areas of the submammary fold.
Technique:
The patient is under general anesthesia. Incision of less than 3 cm periareolar or submammary then access to the edge of the pectoral muscle. Creation of a pocket, most often behind the muscle, whose dimensions are adapted to the projection and diameter of the implant. Disinsertion of the pectoral muscle fibers on the sternum to create a natural neckline (this step allows, according to the patient’s wishes, to create a wide or tight space between the 2 breasts). Next, a type II dual plane is performed: the distal part of the pectoral muscle is freed up anteriorly, up to the height of the areola, in order to reduce the risk of reanimation syndrome (the prosthesis rises when the breast muscle is contracted) and also to have a natural effect when the patient raises her arms (a sliding plane is created between the muscle and the gland and the prosthesis unwinds more smoothly when the patient raises her arms). Insertion of the prosthesis then closure. Dr. Lucas uses biological surgical glue for the scar, so that the patient can take a shower as early as the 2nd day after the operation.
Fat
Under general anesthesia, fat is removed from the knees, thighs, abdomen and hips. The fat is then decanted to purify it, and then reinjected into the breasts to recreate a natural curve.
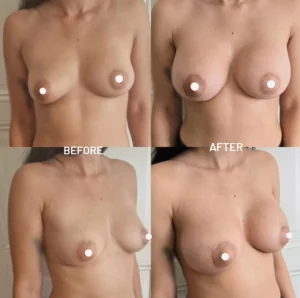
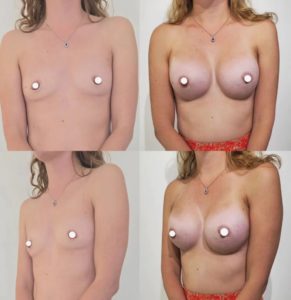
Results :
Time to final results:
2 weeks to see a significant result, 2 to 5 months to see the final result
For patients with small breasts initially, it is often necessary to lower the submammary fold and the skin has a shape memory that fades in a few months. Often, during the first 2-3 months, the breast may appear too bulging in the neckline, then with time, the prosthesis takes place and the upper part of the breast regains a natural shape.
Longevity results :
Definitive, but with weight changes, pregnancies, breastfeeding and time the breast will evolve.
Regarding fat, it is sometimes necessary to perform a second session for an optimal result.
Before surgery :
Stop smoking 1 month before surgery (risk of necrosis of the areola important if active smoking)
Do not take Aspirin 10 days before the operation, inform Dr. Lucas of any anticoagulant medication (Sintrom, Coumadin, Eliquis, etc.) in order to arrange for its discontinuation or replacement.
Take Arnica capsules 5 times a day for 5 days before surgery to prevent hematoma.
Shower with Hibiscrub soap provided on the prescription 48 hours before
No shaving of the axillary zone in the 48 hours before the operation
For patients over 35 years of age or if there is a family history of breast cancer, a screening mammogram should ideally be performed.
On the day of the procedure, you must fast for 6 hours beforehand (do not drink, eat or smoke).
Purchase before the procedure by you of a postoperative bra, the size of which will be specified to you by Dr. Lucas or a girdle, if lipofilling.
Intervention :
Duration of procedure: 1 hour for augmentation with prosthesis / 90-120 minutes for lipofilling / 120 minutes for hydride breast augmentation (implant and fat)
Anesthesia : general
Location: operating room
Outpatient : no hospitalization, no redon
After surgery :
Post-operative pain: 2 to 5/10 the first week, with analgesia by Dafalgan, Irfen and Tramal then after the 1st week, pain to 1/10: painkillers can be gradually stopped. Post-operative pain is significantly reduced because Dr. Lucas performs a pectoral nerve block with a long-acting anesthetic during the operation.
Social eviction: 4-7 days with some discomfort. Shower possible from the 2nd day thanks to the use by Dr Lucas of biological surgical glue replacing the dressings.
Return to work: 7 days
Resumption of sports: 6-8 weeks
Instructions:
Arnica capsules 5 capsules 5 times a day for 5 days after surgery to prevent hematoma.
Permanent cessation of smoking to minimize complications, mandatory if lipofilling
Control Dr Lucas D2, D7, 3 weeks, 3 months, 6 months, 1 year
Implants
During the first 3 days above all: no rapid exertion, rest, do not get up too quickly, take it easy so as not to make any sudden movements (exertion may cause tension to rise and open up the small vessels and thus cause a hematoma)
Compression bandage around the breasts for 24-48 hours, then put in place during the consultation at 2 days of the support bra
Do not lift your arms above 100°, do not carry heavy loads > 3-4 kg and do not push for 6 weeks: the body will form a capsule around the implant during these first 6 weeks, this capsule will accompany you throughout your life. It is essential to respect these instructions during the first six weeks, so that it forms in good conditions.
Bra without underwire 3 weeks day and night, 3 weeks during the day.
Shower from the 2nd day: pass water over the scar without rubbing, dab with clean cloth without rubbing
Between the 2nd day and the 7th day, disinfect the wound once a day with Merfen spray or another disinfectant spray.
From the 15th day, gently rub glue on the scar which will disappear over several days without tearing it off
Bath from 3 weeks depending on the evolution of the scar at 3 weeks.
Massage scar with Gorgonium 2 times 5 minutes per day for 3 months after the shower, from the 15th day.
Strataderm silicone once a day for 3 months, starting on the 15th day.
Sun protection with an index higher than 50 during the 6 months following the surgery.
Follow-up of the scar by Dr. Lucas for 1 year after the surgery is essential.
Lipofilling
Bed rest for 48 hours.
Shower possible from day 3 without rubbing, dab with clean line to dry.
Post-lipoaspiration girdle 2 weeks day and night, 2 weeks day.
Lyman 50 000 IU on fat collection areas 3 times a day to accelerate the disappearance of bruises.
Do not apply pressure on breasts for 3 weeks for a better survival of the fat.
Complications
– Hematoma, seroma: a hematoma can occur especially during the first 48 hours. If it is significant, it is necessary to intervene again and evacuate it. During the first few days, it is necessary to rest and not to make any sudden movements in order to reduce the risk of hematoma.
– Localized skin necrosis, necrosis of the areola: the risk of this is greatly increased by smoking intoxication.
– Infection: fortunately rare, infection may require antibiotic treatment and a new surgical intervention to remove the implants. These can only be put back in place after several months of healing.
– Decreased sensitivity of the areola: often transient, full recovery is generally achieved after a few months.
– Asymmetry
– Rippling (folding of the prosthesis) or feeling of the prosthesis laterally: can be seen in thin patients or after significant weight loss: often transient, but if it remains after 6 months, it can be corrected by lipofilling (fat transfer).
– Abnormal, hypertrophic or even keloid scars: patients with dark skin, at risk of abnormal scars, must pay particular attention to scar care with Gorgonium and Strataderm, follow-up remains essential
– Rupture: rare, often after several decades, rupture requires a change of the implant
– Malposition of the implant: rare, but requires a re-intervention.
– Capsulitis: the capsule formed around the implant follows you throughout your life, until (often after 10-20 years) it becomes inflamed and causes capsulitis. This manifests itself as pain, initially with effort, which gradually sets in at rest. Then, the breast loses its flexibility and in cases of advanced capsulitis, the breast is deformed. When the patient presents pain and the capsulitis is confirmed by imaging (ultrasound or MRI), the implant must be changed and the capsule removed (capsulectomy).
– Breast prostheses and breastfeeding: there are no consequences on breastfeeding, the patient can breastfeed after a breast augmentation by prosthesis.
– Scar dehiscence and delayed healing (favored by smoking): sometimes there are small openings of the scar of a few millimeters, which can be treated with dressings usually without the need for reoperation. The follow-up of the scar by Dr Lucas is essential.
– Concerning lipofilling, calcifications can be seen on the images after breast lipofilling: not pathological, but the images for breast cancer follow-up must be read by a radiologist who is used to it, preferably in a breast center. Secondly, lipofilling presents the usual risks of liposuction.
Combinations and alternatives
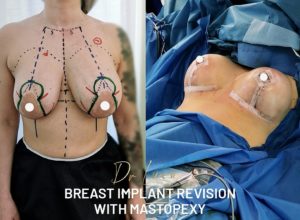
When the sagging (ptosis) and excess skin are too great, a breast lift or mastopexy should be combined with the procedure. The size of the nipples can be increased at the same time by fat transfer.